Exploring Neurogenic Thoracic Outlet Syndrome
by Robert Tallitsch, PhD | July 27, 2021

Watch this 3 minute video for a simplified explanation of Neurogenic Thoracic Outlet Syndrome including symptoms, causes, treatments, and a real patient example based on Brandon's story!
During my 43 years at Augustana I always had an “open door” policy with my students. I never posted office hours. If a student wanted to talk they just dropped by my office to see if my door was open. If another student wasn’t already there they could walk in, talk, and ask questions about anything — course related or not.
Brandon was a second-year pre-medicine major and butterflier on Augustana’s swim team. He won the 200 and 400 yard individual medley and the 100 and 200 yard butterfly events in conference. He also qualified for DIII NCAA nationals and earned All American status in 3 events. He was still practicing, hoping to qualify for a high-power training team in Boulder Colorado for the summer. He was in Human Anatomy and stopped to talk about enrolling in Neuroanatomy the next term. Brandon had just completed this week’s swim drills and weight training and was perplexed by recurring neck and shoulder pain and a tingling in his upper limb and fingers. When I asked him to squeeze my “stress ball” he complained that one hand seemed stronger than the other. I urged Brandon to see the team doctor to get evaluated, and to keep me posted as to the diagnosis and recommended treatment. At the end of the term Brandon informed me that he was diagnosed with neurogenic thoracic outlet syndrome (nTOS), and was scheduled for surgery during break between tri-semesters. We talked at length about the structures that were causing his nTOS.
To understand nTOS one needs to understand three concepts: the brachial plexus, the superior thoracic outlet, and how compression of these structures causes nTOS.
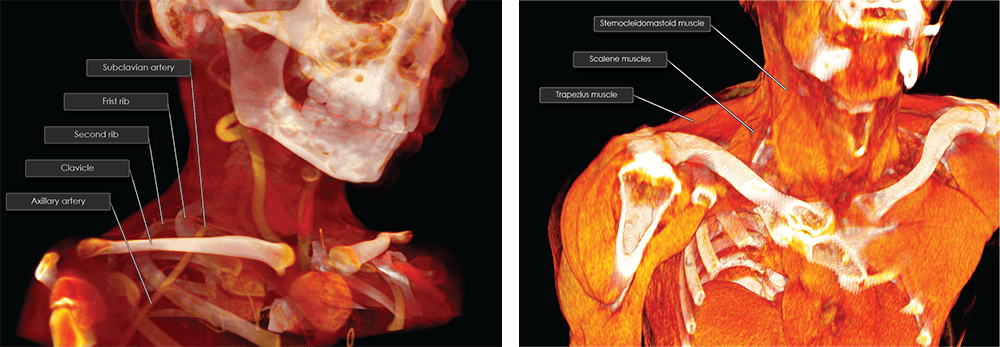
Most of the nerves of the pectoral girdle and upper limb originate in the brachial plexus, which originates from the ventral rami of spinal nerves C5 to T1. These ventral rami unite to form the roots of the brachial plexus, and these roots pass between the anterior and middle scalene muscles as they exit the superior thoracic outlet (STO).
C5 and C6 roots unite to form the superior trunk. The C7 root continues as the middle trunk, while C8 and T1 roots unite to form the inferior trunk. These trunks then divide forming anterior and posterior divisions. The three posterior divisions unite, forming the posterior cord. The anterior divisions of the superior and middle divisions unite and form the lateral cord. The anterior division of the inferior trunk continues as the medial cord. (The cords are named according to their relationship to the axillary artery.) The fifteen nerves of the brachial plexus arise from one or more of these trunks or cords.
Structures passing from the thoracic cavity into the neck or upper limb pass through the kidney-shaped STO. The STO is bounded posteriorly by the first thoracic vertebra, anteriorly by the superior border of the manubrium, and laterally by the first ribs and their costal cartilages.
Thoracic Outlet Syndrome (TOS) is clinically described as neurological or vascular symptoms within the upper limb due to compression of the neurovascular bundle in the STO superior to the first rib. nTOS comprises 95% of all TOS patients, venous TOS comprises 4%, and arterial TOS 1%. TOS is often caused by repetitive movements, vocational over-use injuries, or trauma (typically hyper-extension of the neck). It is also seen in high-performance athletes in sports involving overhead, rapid upper-limb movements, such as swimming or baseball. These muscular movements result in hypertrophy of the anterior and middle scalene muscles, a narrowing of the STO, and compression of either the neural or vascular structures passing through the STO.
The STO has three spaces that are potential sites for neurovascular compression: (1) the interscalene triangle, (2) costoclavicular space, and (3) the subpectoralis minor space.
The interscalene triangle is formed anteriorly by the anterior scalene muscle, posteriorly by the middle scalene muscle, and inferiorly by the first rib. There are three common compression scenarios within the interscalene triangle (not including the presence of a costal rib) that result in TOS.
- The anterior and middle scalene muscles are accessory muscles of respiration. They elevate the first rib, flex the neck and, with unilateral contraction, laterally flex and rotate the neck to the opposite side (anterior scalene) or same side (middle scalene). These muscles insert on the first rib. The insertions form a “V” formation if they overlap, creating a narrow space. This places the subclavian artery and the brachial plexus in a higher than normal position, making them susceptible to compression injuries.
- Sometimes the middle scalene inserts along the entire length of the first rib, creating a narrow space through which the neurovascular structures must pass.
- Finally, the scalene muscles may intermingle proximally, creating a small space that will exert pressure on the brachial plexus from above.
Compression of the brachial plexus and/or the subclavian artery within the costoclavicular space is often the result of trauma or congenital abnormalities to the first rib and/or clavicle. The costoclavicular space is triangular, bordered posterolaterally by the superior border of the scapula, posteromedially by the first rib and the insertions of the anterior and middle scalene muscles, and anteriorly by the medial segment of the clavicle and the underlying subclavius muscle.
Compression within the subpectoral minor space is quite rare. This space is inferior to the coracoid process and deep to the pectoralis minor insertion. The pectoralis minor muscle compresses the vascular structures inferior to the coracoid process during hyperabduction of the upper limb.
Brandon’s surgery to alleviate his nTOS was successful, and he returned to full competitive activity within 3 months. He had an even more successful swimming season during his third year at Augustana, reaching All American status in five events at the NCAA DIII national meet.
Additional Articles: