Liver Transplantation From A Living Patient
by Robert Tallitsch, PhD | August 26, 2021

Short video explanation of the difference between a living liver transplant and normal liver transplant with symptoms, causes, treatments and a patient case example of liver failure!
In our anatomy courses, it is almost impossible to talk about the anatomy of a structure without reviewing its function. This often leads to a discussion about the consequences of organ failure and the importance of being an organ donor — yet another real-world connection we have at our disposal as anatomy educators.
To engage my students further, I like to point the discussion towards being a “living donor” by mentioning how a former student of mine donated one of his kidneys to a friend. I remember one class where the topic just took off, prompting one of those times when you throw away the daily syllabus to follow your students’ interests and tie it back to the course concepts. We talked about the lack of organ donors and how, on average, 20 U.S. citizens die every day while waiting for an organ transplant. This, in turn, led into the discussion of how some children, who cannot survive without a new liver, receive their new liver not from a deceased, cadaveric donor but from a living individual — usually a relative. We then found ourselves comparing the gross anatomy of the liver to the surgical anatomy of the liver — a topic that I hadn’t considered spending a lot of time on that day.
Although these topics weren't necessarily a part of my syllabus for the day, I was more than happy to spend our class session discussing these topics. As any anatomy educator knows, it can be extremely difficult to engage your students at times, so when you find a topic they're interested in it is best to embrace it. So, let’s talk about the gross anatomy of the liver, the surgical anatomy of the liver, and how (with today’s technology) we are able to perform a liver transplant from a living donor.
Gross Anatomy of the Liver
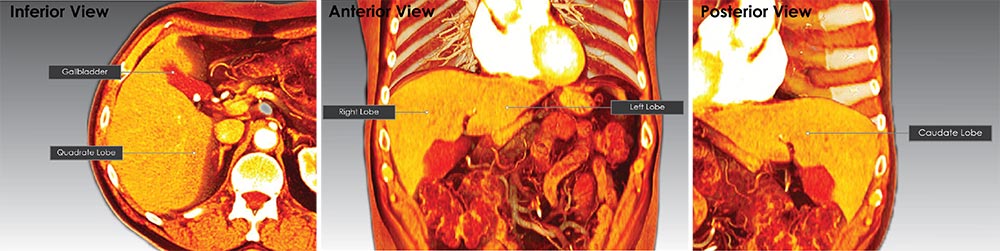
The liver is the largest gland in the body, weighing approximately 1500 grams, or 2.5% of average body weight! The liver occupies the right hypochondriac, epigastric, and part of the left hypochondriac abdominal regions, lying immediately inferior to the diaphragm. The intraperitoneal organ is suspended from the diaphragm by the coronary ligament. Viewing the liver, you note that it is divided into four lobes. The right and left lobes are separated by the falciform ligament. The quadrate lobe is seen left of the gallbladder on the inferior surface of the liver. The fourth lobe is the caudate lobe, found on the posterior surface of the liver surrounding the inferior vena cava. Gross anatomists state that the liver is subdivided into two main lobes (right and left) and two accessory lobes (quadrate and caudate).
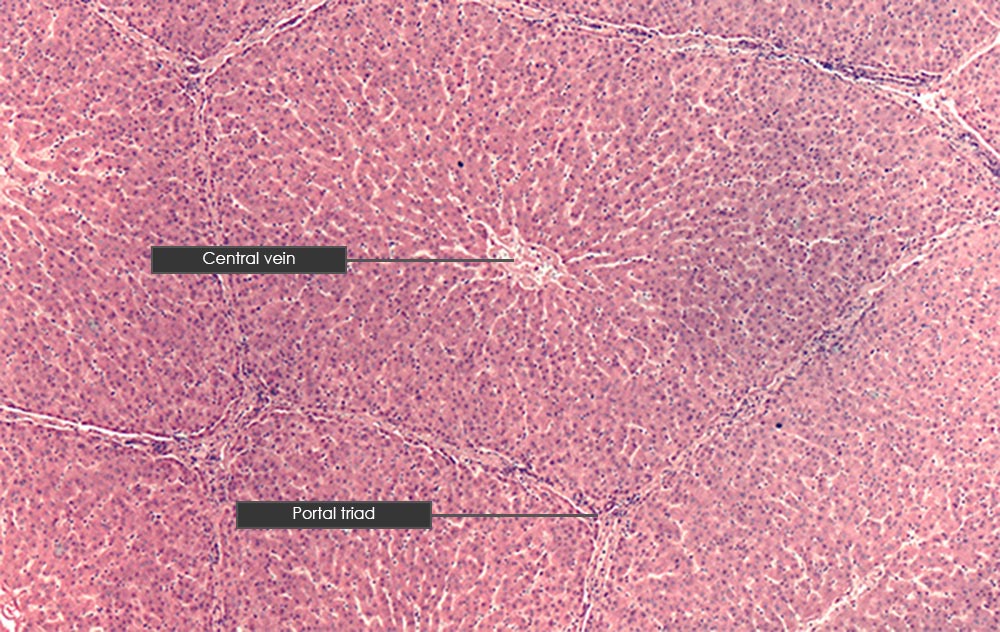
Histologically, the functional unit of the liver is the hepatic lobule (or liver lobule), and an adult liver will have approximately 100,000 of these functional units. The cells of the liver, termed hepatocytes, are arranged like spokes of a wheel radiating out from a central vein. Blood enters the liver via the hepatic artery proper and the hepatic portal vein. Blood ultimately flows into highly fenestrated capillaries termed hepatic sinusoids, which completely surround the hepatocytes. Blood then drains into the central vein of the hepatic lobule; the central veins converge to form the hepatic veins, which drain blood from the liver into the inferior vena cava. A hepatic lobule is six-sided. At each of the six corners of the lobule one finds a portal triad, which is composed of (1) an interlobular artery, (2) an interlobular vein, and (3) an interlobular bile duct.
Surgical Anatomy of the Liver
The understanding of the surgical anatomy of the liver has changed considerably throughout the years. Autopsy observations, and results from experimental surgical procedures, changed the process by which the internal and external lobes of the liver were identified. These changes in the surgical anatomy of the liver were all based on trying to better guide surgeons, thereby increasing the survival rate from hepatobiliary surgeries. Sadly, this expansion of naming schemes for the liver’s lobes resulted in more confusion than clarity, until Couinaud’s system of identifying liver segmentation was adopted and refined by the surgical community in the late 90s. Couinaud’s system is based on the underlying principle that each segment of the liver has an independent vascular input, output, and biliary drainage. The liver is divided into hemilivers, sectors and segments (in order of descending magnitude), resulting in nine segments: 1, 2, 3, 4a, 4b, 5, 6, 7 and 8. This can be quite confusing at first encounter, even for a trained anatomist, so for some excellent visual representations of Couinaud’s system see the reference cited at the end of this article.
Living Liver Transplantation
But how does this tie into liver surgery and transplantation? Initially, Couinaud’s concept of segmental hepatic anatomy allowed for the removal of cancerous segments of the liver based on the size and location of a cancerous lesion. This produced liver resections with minimized surgical blood loss and postoperative necrosis of tissue. Because the liver is the only organ capable of regeneration, these surgical findings led to new surgical techniques for pediatric liver transplantations. Couinaud’s system first allowed for a reduced-size liver transplantation utilizing only a segment of the liver rather than the entire liver from a cadaveric donor. This enabled the donor liver to fit into the smaller abdominal cavity of the child. Living liver transplantation was the logical extension of reduced-size liver transplantation from cadavers and is the most recent achievement in the evolution of surgical procedures involving the Couinaud’s system.
A living liver transplantation was first accomplished in 1989. Today, thanks to the Couinaud system of understanding the surgical anatomy of the liver, living-related liver transplantation is accepted as an effective procedure in liver transplantation, and is performed in many surgical centers throughout the world. This type of liver transplantation has several advantages, both theoretical and immediate, as compared to the utilization of cadaveric donors. First, waiting time for a suitable donor is reduced. In addition, the minimalization or elimination of medical deterioration in the patient while waiting for a suitable donor is reduced or eliminated. Finally, the transplantation procedure can be performed when the recipient’s health is optimal rather than at a time dictated by the availability of a suitable cadaveric donor.
Topics like this help to explain the differences between gross anatomy and surgical anatomy — something that students of anatomy may not realize until much later in their academic career. Engaging your students with interesting stories and real-world connections helps ensure they carry these topics with them throughout their academic and professional careers.
Additional Articles: